 +919674493673
+919674493673  mailus@wbcsmadeeasy.in
mailus@wbcsmadeeasy.in






















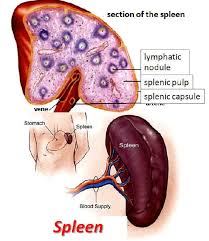
Splenomegaly – Medical Science Notes – For W.B.C.S. Examination.
স্প্লেনোমেগালি – মেডিকেল সায়েন্স নোটস – WBCS পরীক্ষা।
Splenomegaly is almost always secondary to other disorders. Causes of splenomegaly are myriad, as are the many possible ways of classifying them.Continue Reading Splenomegaly – Medical Science Notes – For W.B.C.S. Examination.
Infectious diseases (eg, malaria, visceral leishmaniasis)
If splenomegaly is massive (spleen palpable 8 cm below the costal margin), the cause is usually chronic lymphocytic leukemia, non-Hodgkin lymphoma, chronic myeloid leukemia, polycythemia vera, primary myelofibrosis, Gaucher disease, or hairy cell leukemia.
Splenomegaly can lead to cytopenias, a disorder called hypersplenism.
Evaluation
History
Most of the presenting symptoms result from the underlying disorder. However, splenomegaly itself may cause early satiety by encroachment of the enlarged spleen on the stomach. Fullness and left upper quadrant abdominal pain are also possible. Sudden, severe pain suggests splenic infarction. Recurrent infections, symptoms of anemia, or bleeding manifestations suggest cytopenia and possible hypersplenism.
Physical examination
The sensitivity for detection of ultrasound-documented splenic enlargement is 60 to 70% for palpation and 60 to 80% for percussion. Up to 3% of normal, thin, people have a palpable spleen. Also, a palpable left upper quadrant mass may indicate a problem other than an enlarged spleen such as a hypernephroma.
Other helpful signs include a splenic friction rub and shoulder pain that suggest splenic infarction as well as epigastric or splenic bruits that may occur due to increased blood flow. Adenopathy may suggest a lymphoproliferative, infectious, or autoimmune disorder.
Testing
If confirmation of splenomegaly is necessary because the examination is equivocal, ultrasonography is the test of choice because of its accuracy and low cost. CT and MRI may provide more detail of the organ’s consistency. MRI is especially useful in detecting portal or splenic vein thromboses. Nuclear scanning is accurate and can identify accessory splenic tissue often found after splenectomy due to “work hypertrophy” of overlooked splenules at the time of surgery.
Specific causes suggested clinically should be confirmed by appropriate testing. If no cause is suggested, the highest priority is exclusion of occult infection, because early treatment affects the outcome of infection more than it does most other causes of splenomegaly. Testing should be thorough in areas of high geographic prevalence of infection or if the patient appears to be ill. Complete blood count (CBC), blood cultures, and bone marrow examination and culture should be considered. If the patient is not ill, has no symptoms besides those due to splenomegaly, and has no risk factors for infection, the extent of testing is controversial but probably includes CBC, peripheral blood smear, liver tests, and abdominal CT. Flow cytometry and immunochemical assays such as light chain measurements of peripheral blood and/or bone marrow sections is indicated if lymphoma is suspected. Lymphoma in the splenic marginal zone, which is uncommon, is often associated with hepatitis C infection (and is important to detect because it can be successfully treated with viral eradication).
Specific peripheral blood findings may suggest underlying disorders (eg, small-cell lymphocytosis in chronic lymphocytic leukemia, large granular lymphocytosis in T-cell granular lymphocyte [TGL] hyperplasia or TGL leukemia, atypical lymphocytes in hairy cell leukemia, and leukocytosis and immature forms in other leukemias). Excessive basophils, eosinophils, or nucleated or teardrop RBCs suggest myeloproliferative neoplasms. Cytopenias suggest hypersplenism. Spherocytosis suggests hypersplenism or hereditary spherocytosis. Target cells and spherocytes can suggest a hemoglobinopathy.
Liver test results are diffusely abnormal in congestive splenomegaly with cirrhosis; an isolated elevation of serum alkaline phosphatase suggests hepatic infiltration, as in myeloproliferative and lymphoproliferative disorders, miliary tuberculosis, and chronic fungal diseases (eg, candidiasis, histoplasmosis).
Some other tests may be useful, even in asymptomatic patients. Serum protein electrophoresis identifying a monoclonal gammopathy or decreased immunoglobulins suggests lymphoproliferative disorders or amyloidosis; diffuse hypergammaglobulinemia suggests chronic infection (eg, malaria, visceral leishmaniasis, brucellosis, tuberculosis) or cirrhosis with congestive splenomegaly, sarcoidosis, or connective tissue disorders. Flow cytometry can identify a small monoclonal lymphocyte population suggestive of lymphoma. Elevation of serum uric acid suggests a myeloproliferative or lymphoproliferative disorder. Elevation of leukocyte alkaline phosphatase (LAP) suggests a myeloproliferative neoplasm, whereas decreased levels suggest chronic myelocytic leukemia.If testing reveals no abnormalities other than splenomegaly, the patient should be reevaluated at intervals of 6 to 12 mo or when new symptoms develop.
Treatment
Treatment of underlying disorder
Treatment is directed at the underlying disorder. An enlarged spleen itself in an asymptomatic patient needs no treatment unless severe hypersplenism is present. Patients with palpable or very large spleens probably should avoid contact sports to decrease the risk of splenic rupture.
Please subscribe here to get all future updates on this post/page/category/website